Tooth loss is systematically accompanied by alveolar bone loss
Therefore, implant placement often requires a prior bone volume augmentation step. Many surgical techniques exist, including the onlay graft. The procedure and protocol .
Thank you for visiting our website.
This site is exclusively reserved for health professionals.

I am a health professional

I want to access the \“patient\” website
Tooth loss is systematically accompanied by alveolar bone loss
Therefore, implant placement often requires a prior bone volume augmentation step. Many surgical techniques exist, including the onlay graft. The procedure and protocol .
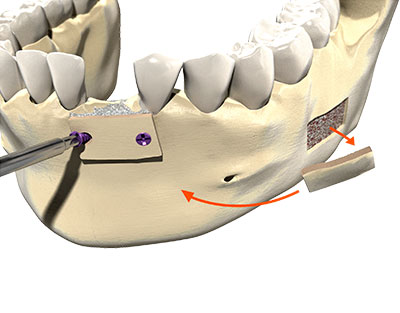
This surgical technique, described in 20th century literature, consists of applying an autologous or heterologous bone graft to the bone defect to be restored using an osteosynthesis screw.
Objective
The objective of the technique is to replace enough volume in the bone crest for placement of dental implants, respecting the 5 mm rule, by bone block fixation. The bone block may be autologous (harvested from the recipient patient) or heterologous (source other than the recipient: human, animal or synthetic) in origin.
Advantages
Limitations
The success of a bone graft depends partly on the surgical technique used, but this is not the only consideration. For onlay grafts, the following points apply:
Preparation of the recipient site
The recipient site is the entry point for healing of the graft and must bleed so that the graft is rapidly saturated with blood. This step can be completed in several ways, notably by:
Adaptation and preparation of the bone graft
Healing of a bone graft always occurs via establishment of a fibrin network to ensure good graft stability. This is assured via establishment of neovascularisation and integration of the bone block. The three essential steps for satisfactory preparation are as follows:
Closure of soft tissues without tension
A sufficient volume of residual bone is required at the site for graft fixation. Pay attention to the interradicular spaces for the fixation screws.
Protocol: